
Early on in neurosurgery residency, we are introduced to something called a perforator drill. This is a relatively safe drill bit because it is meant to create a burr hole in the skull and automatically stop before the dura. It’s supposed to be safe, but as residents we always find a way to make attendings cringe. How can we do this? This can be done by not understanding how something works. A lack of understanding doesn’t mean it won’t work, but understanding how it does can add an extra layer of safety. Mainly, don’t use the drill inappropriately and there will be less of a pucker factor.
Below is a picture of a Medtronic perforator drill bit. I have no financial stakes in Medtronic, it’s just they were the ones who put on a course for me to experiment with the drills and bits (on non living tissue) so my pictures and understanding are based on this experience.
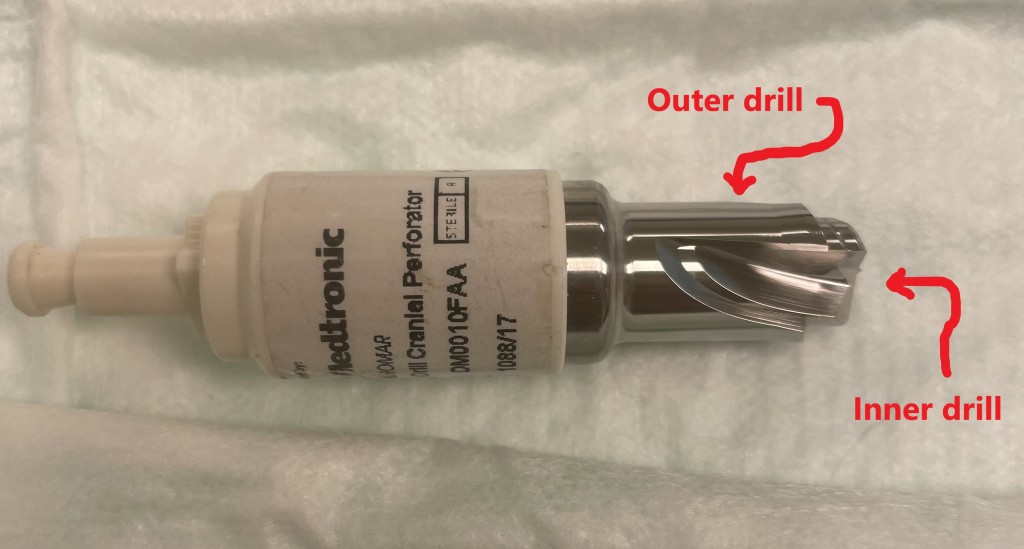
The drill bit consists of an inner and outer drill. I’m sure there are some differences among different companies. In general, the inner drill must be depressed for the outer drill to spin against resistance. As a corollary this means if the inner drill is not depressed the outer drill will not spin against resistance. I add the term resistance because if you step on the drill pedal when the drill is not touch anything both the inner and outer drills will be spinning. https://pagead2.googlesyndication.com/pagead/js/adsbygoogle.js (adsbygoogle = window.adsbygoogle || []).push({});
To start some people will tell you that you must start with the drill engaged on the surface of the bone before stepping on the pedal. Other attendings tell me to step on the pedal prior to engaging the surface of the bone. My best guess as to the differences is in how they were trained and possible the workings of these drills in earlier generations of the inner and outer drilling mechanism. What I can say is that having tried both ways, they both work.
As a resident I’ve also been told, “don’t take your foot off the pedal” until the drill stops on its own. If you take your foot off the pedal before getting through the skull then it will not work. Once again, I assume this might be based on earlier iterations of the drill or prior experiences. Currently after playing, sorry working with the perforator in the lab, if you stop midway, you can still step on the pedal again and it will engage. As long as there is something to apply pressure to the inner drill then both the inner and outer drill will spin against resistance.
Something everyone seems to agree on though is that the drill should be started at a perpendicular/orthonormal position to the surface of the skull. It is not impossible to start the drill at a different angle but the smooth surface of the skull can lead to the drill slipping to a different position than the one intended if angled.
Once the drill gets through the outer table of cortical bone the drill will continue until the inner drill does not experience enough counter pressure to keep the inner drill engaged. So theoretically if the diploe (layer between inner and outer cortical bone) is soft, it might not provide enough resistance to the inner drill which could lead to the outer drill stopping and therefore entire drill not advancing. I have not experienced this however it could be a reason for premature stopping.
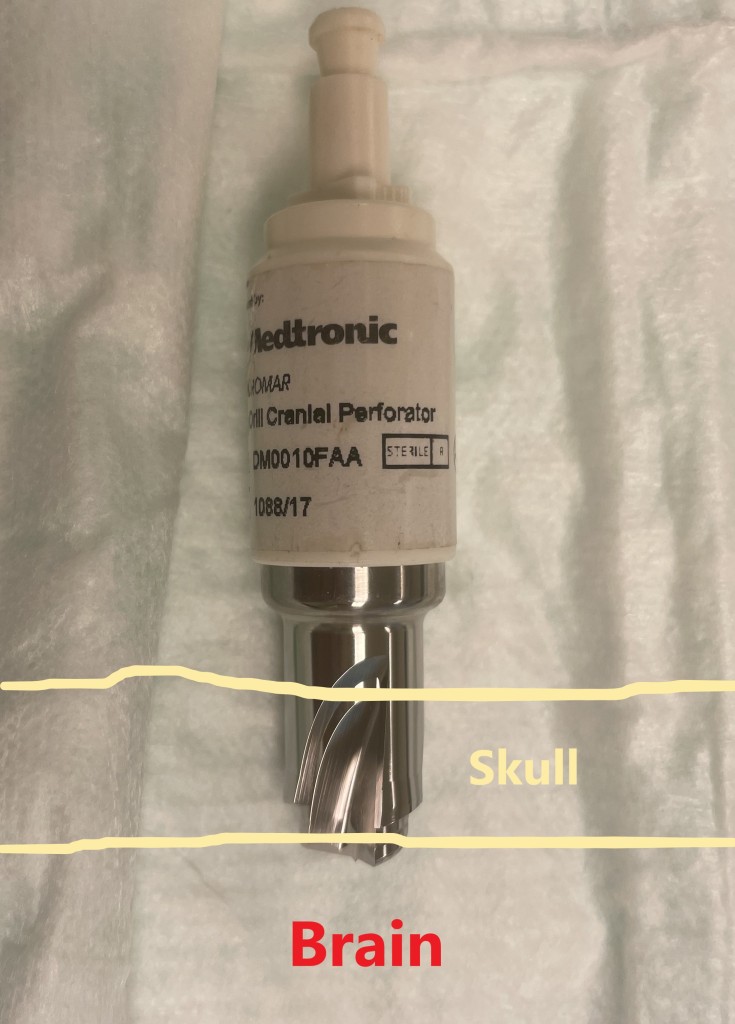
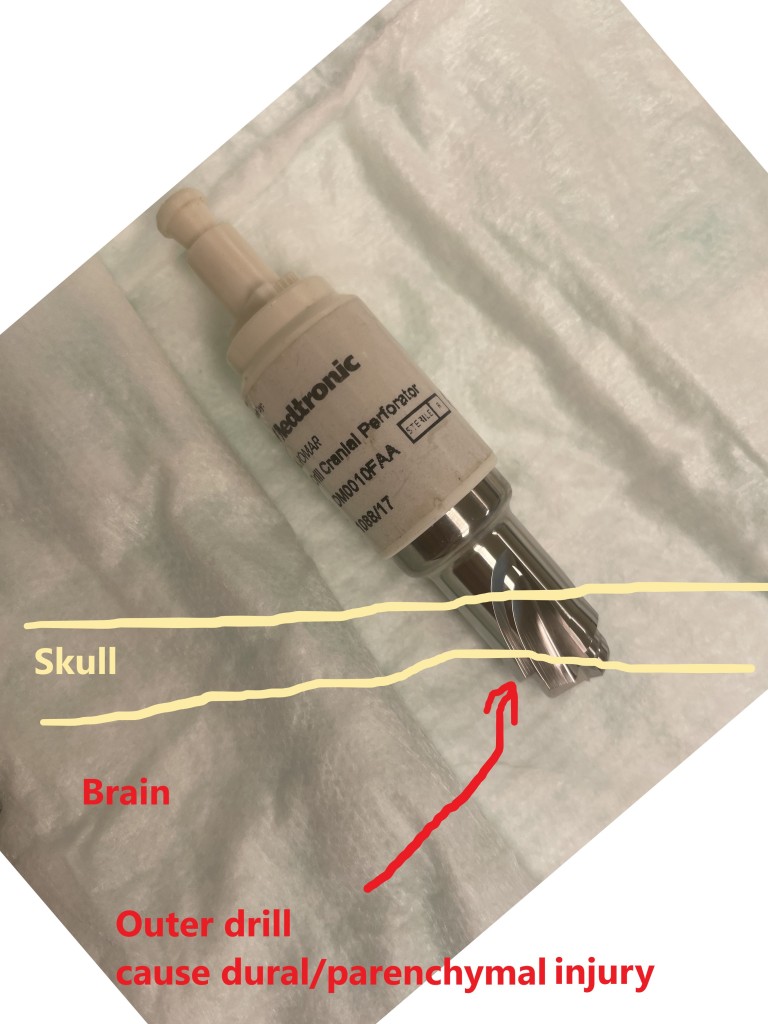
While the drill is advancing the manufacturers do NOT recommend precessing the drill. Changing the angle of the drill while advancing can prevent the drill from reaching the inner cortical bone at an orthonormal angle. Reaching the inner table at an orthonormal angle is important because when the inner drill advancing through the inner table at this angle the entire inner drill has cleared the bone and the opposing pressure drops off such that the outer drill will stop preventing the entire drill from advancing further. If the inner drill violates the inner table at an angle, the inner table may be partially violated, but the outer drill will continue allowing the entire drill to advance. If this continues the outer drill can cut the dura or even parenchyma depending on how far it advances. The outer drill will not stop until the inner drill has advance through enough of the inner cortical bone where it does not provide enough resistance to keep inner drill engaged. Attempts at pictoral representations shown below.
So I’m safe as long as I’m orthonormal? Not necessarily. Some bones are abnormally shaped along the inner surface. This could mean the drill might not disengage at the desired location. Therefore it is worth evaluating pre op imaging to determine if that might be a potential pitfall. Also the thickness of bone makes a big difference. These perforator drills come with measurements. The measurements are typically three numbers (ex 14mm x 11mm x 1mm). The first number indicates the outer diameter (outer drill). The second number indicates the inner diameter (inner drill). The last number indicates the shelf or the depth difference (superficial to deep) between the inner and outer diameter when the drill disengages. The diameter numbers are useful in selecting the size of the burr hold depending on the intended procedure. It lets you know if you can fit other instruments like a Kerrison rongeur or a catheter through the hole. The shelf is a helpful in letting you know how thick a bone “should” be. For instance, if the shelf rating on a perforator is 4mm and the you decide to make a burr hole on the squamous temporal bone that is only 2mm thick. You could theoretically damage the underlying parenchyma before the drill stops. Not all companies show the third number, but the rep at the course for this particular company explained what the numbers on their bits stood for. Another company shows the sizing things in video format on youtube.
The video below is interesting in that the surgeon introduces the perforator into a burr hole in which it had already stopped. As you can see the perforator did not spin again since the inner drill did not contact a surface hard enough to engage the outer drill.
Below a paper saying that brain can be injured from the use of these drills. Hopefully the above explains some of the limitations of using the these drills bits and leads to improved safety.
https://thejns.org/view/journals/j-neurosurg/115/3/article-p570.xml
