Placement of screws during spine surgery is a common practice. The manner in which the screws are placed can range from “free hand” where a surgeon cannulates the desired path by feel and then subsequently places the screw to using intraoperative navigation. Today’s post is about the differences in images obtained from fluoroscopy and CT.
CT is often used preoperatively for planning screw sizes. Below the axial images obtained at L2 for a planned posterior instrumentation and fusion.


The above image shows the upper limits for the planned screw size characteristics. During the case 4.0mm x 45mm screws were selected. An intraoperative image is shown below.
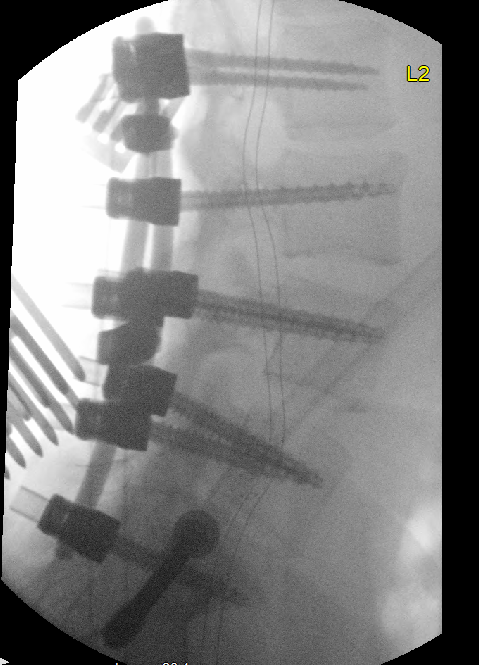
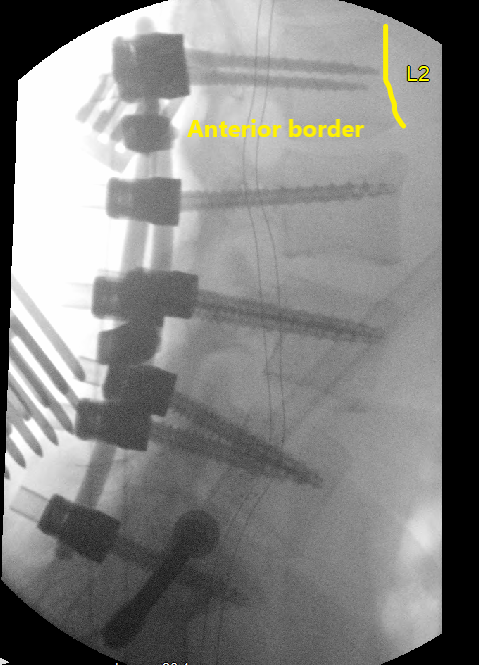
When looking at the L2 screws on the intraoperative image, they appear to be “short” since they do not pass the anterior border of the vertebral body. However a CT that was obtained of the abdomen post operatively demonstrates the screws have just started to break through the opposing cortex.

I point out these images because it shows the differences between intraoperative imaging obtained with a C arm (pretty much an XR) vs a CT scan. A CT scan shows individual slices whereas the XR is a summation of all those slices “compressed” into a single image. Therefore it is possible to breakthrough the anterior border of the vertebral body even though the screw does not appear to be past the anterior border of the vertebral body on XR.
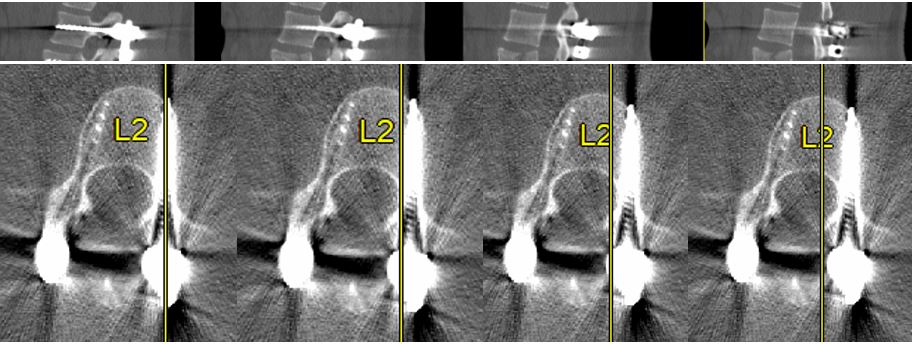
In an attempt to show this another way, below are a series of sagittal images coming from more lateral on the left to medial on the right. The yellow line on the axial images shows the respective position of the sagittal image above. The left most image shows the screw just breaking through the anterior border of the vertebral body. However, as the images are shifted more medial the anterior wall is “more forward” than the anterior wall on the lateral slices. This is due to the rounded shape of the anterior wall of the vertebral body. If we overlay all the sagittal images on top one another we would get an XR image. Therefore in the OR if relying solely on the anterior border as viewed through the XR the screw may violate the anterior border despite the surgeon feeling confident in placement. This is a big deal especially if there are vascular structures like the aorta, or vena cava overlying the area where the screw could break through.
So my saying preoperative planning is important, that is not new or earth shattering. However, I think it is worth recognizing the limitations of an intraoperative XR when using it to guide screw placement.
Moral of the story: intraoperative XR is a 2D representation of a 3D structure, therefore be cognizant of the limitations of this image guidance when placing screws.
