
The term kind of sounds like a superhero or villain. Their super power is to alter perspective. Almost sounds like mind control, or the power of illusion. Maybe Parallax can be a magician like Doctor Strange.
Edit: upon further review there already is a comic book villain in the DC universe called Parallax.
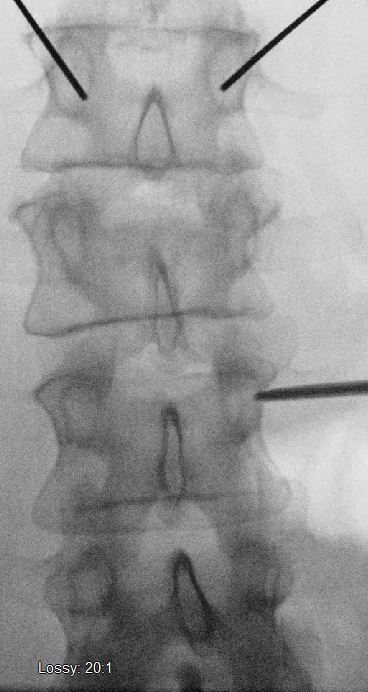
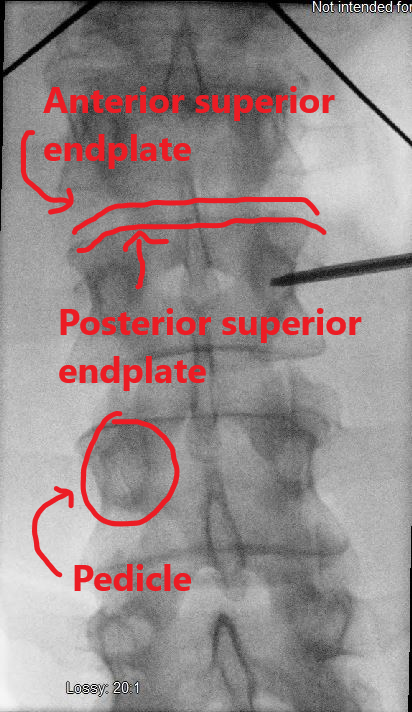
Anyway, parallax refers to a difference in positional appearance due to a shift in viewing angle. During spine cases this becomes important when localizing using C arm. Often times a C arm is used to identify pedicles for screw placement. If you look at the picture below one might assume this is a suboptimal position since it is a starting point somewhat in or near the inferior medial quadrant.

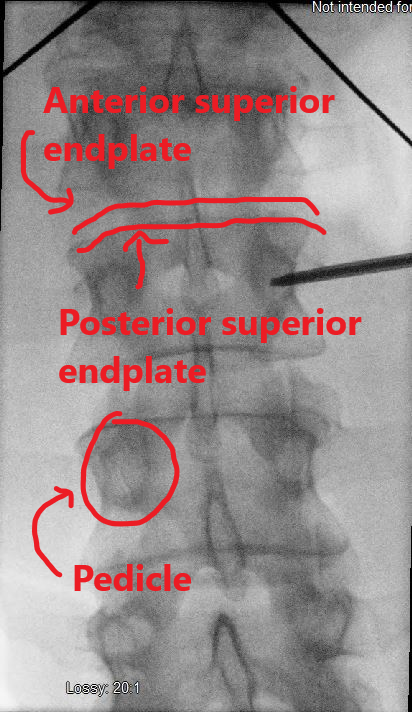
Just for reference above picture with labels is found below.
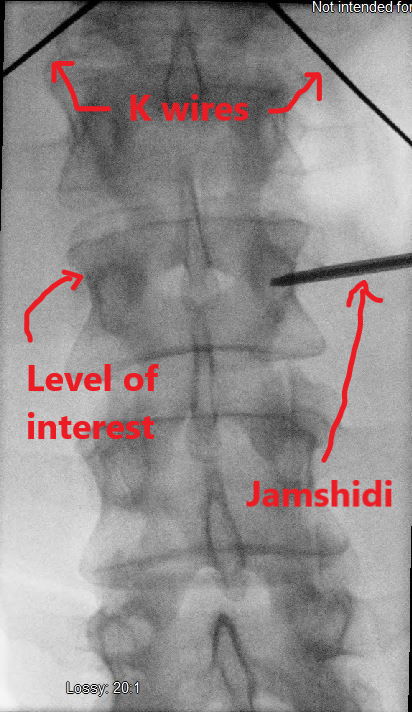
This apparent position for ideal starting point depends on the position of the C arm. If you look further at the image above you can see that the endplates aren’t aligned at the level of interest. Below is a labeled the same image.
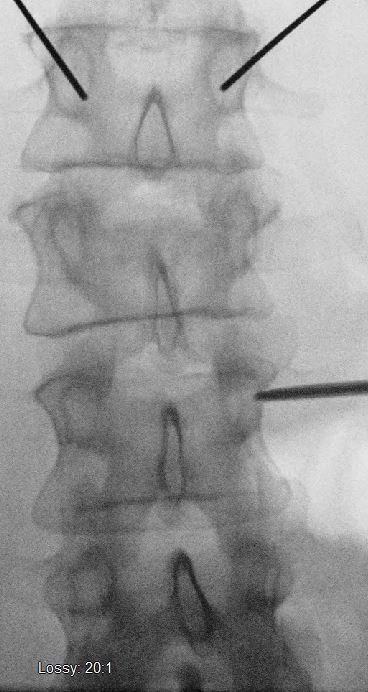
So why does angle matter? Well let’s change the angle of the C arm to align the endplates.
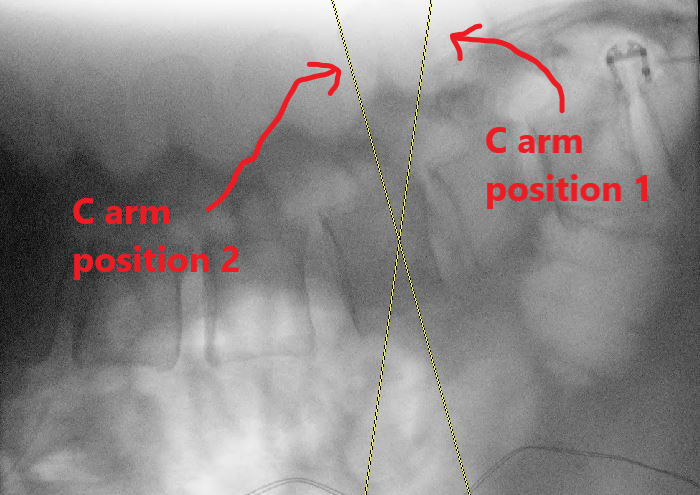

The below image is taken with the Jamshidi and K wires in the same position, but the C arm Ferguson angle changed as shown between the two pictures above.
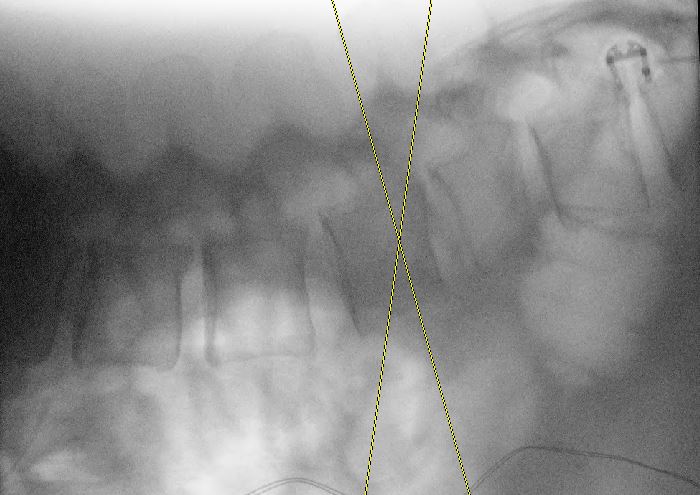
This time, reviewing the image, the Jamshidi is in the upper outer quadrant in a position closer to 3 o’clock. This is PARALLAX the supervillain responsible for screws going astray. However, the surgeon is still responsible regardless of whatever villains, techs, reps, or junior residents may try to sabotage our case. These are all valuable members of the team and I’ve noticed good reps are able to gently remind surgeons of potential errors. That being said while reps have a vast amount of experience, do not underestimate your medical training. You provide a unique view that should not be ignored. Patient outcomes trump all. Anyway, repositioning the C arm resulted in this shot above. The superior endplate is better aligned. So what? If I stay in the pedicle regardless of C arm position then my screw won’t breech the canal. While this is somewhat true consider this. A screw is straight therefore its trajectory can be defined by two points. One of those points I’m assigning to the middle of the pedicle because we don’t want to breech the pedicle. *There are techniques where you may do fancy things where you intentionally place a screw lateral to the pedicle or breech laterally intentionally, but I’m a resident so you’ll have to look at other websites for that stuff* The other point for the screw trajectory I’m assigning as the starting point. If you look at the picture below, the lines represent different trajectories based on starting points and the middle of the pedicle.

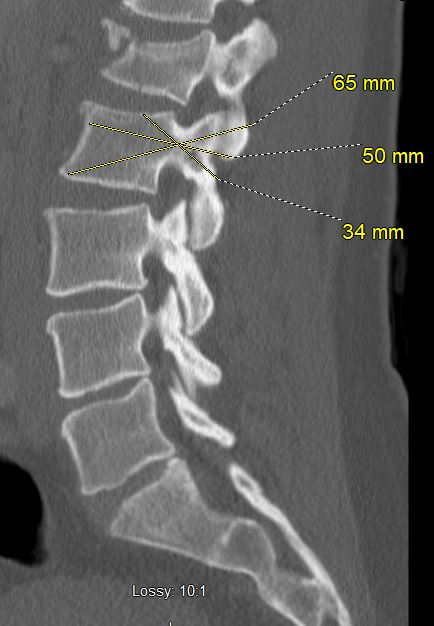
While the above pictures are exaggerations for starting points, I’m just trying to demonstrate that the starting point makes a difference even if you stay in the pedicle. This also becomes apparent in percutaneous cases where your preoperative screw measurements may not coincide with the trajectory which your screw is committed to based on intraoperative imaging. Therefore, you may end up with breeches through the vertebral body. It’s still possible to switch the C arm between AP and lateral views to correct the trajectories and ensure proper screw placement. However, setting ourselves up for success from the beginning will save time which ultimately means shorter anesthesia time for patient and less frustration for operative team.
Anyway, since COVID has cut down on case numbers I can participate in, I’ve had more opportunity to do posts which is helpful for me in terms of learning since I have to explain it in a hopefully useful way to others. Feedback is appreciated. Below are some screw placement pictures because I was allowed to place the patient’s right sided screws (under direct supervision during which the attending was scrubbed and performed all critical aspects of the case. All sponge and needle counts were correct x2.). Punctuation looks weird. Good thing this isn’t going through a journal for peer review.
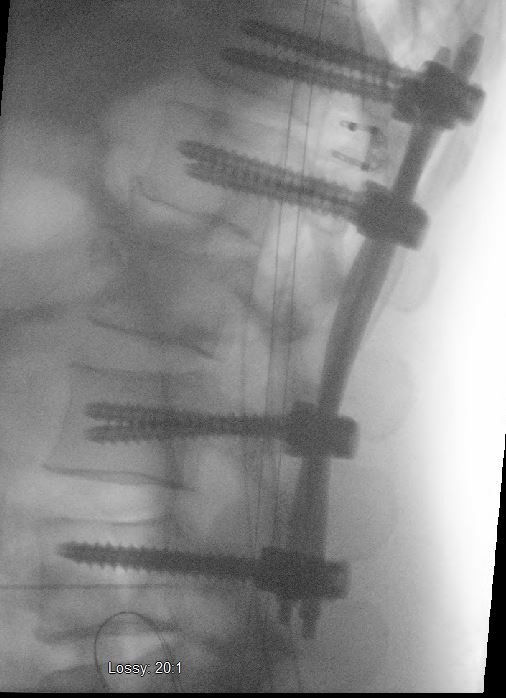
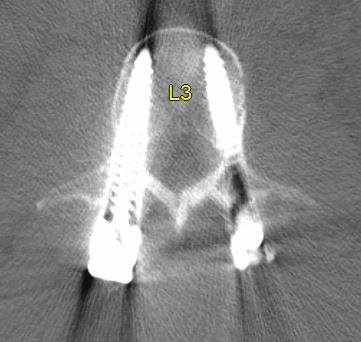
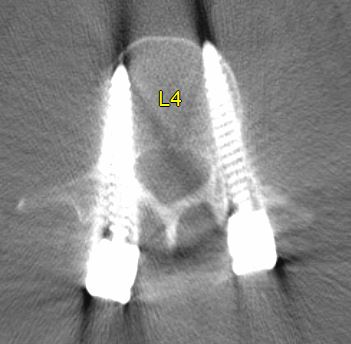
Pictures below are in “normal” orientation where the patient’s right is on the left side of the picture.
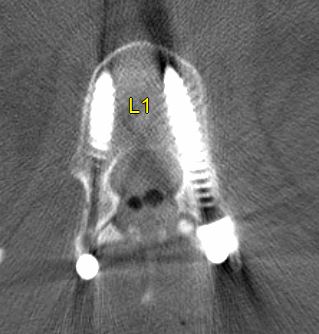
We skipped L2 the fractured level. Did a laminectomy at this level.

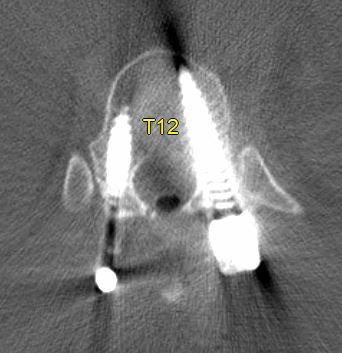
Please don’t burn us for “wrong level” surgery. The patient has 6 lumbar vertebrae based on the last rib attaching to T12 (patient had 12 ribs on each side).
EXTRA CREDIT:
Extra credit may be redeemed in your OR for avoiding complications like nerve root injuries or central canal breeches/dural leaks.
As shown in the below picture the superior endplates are not well aligned.
After changing the position of the C arm, the superior endplates look slightly better but the inferior endplates look a little less aligned as shown below.
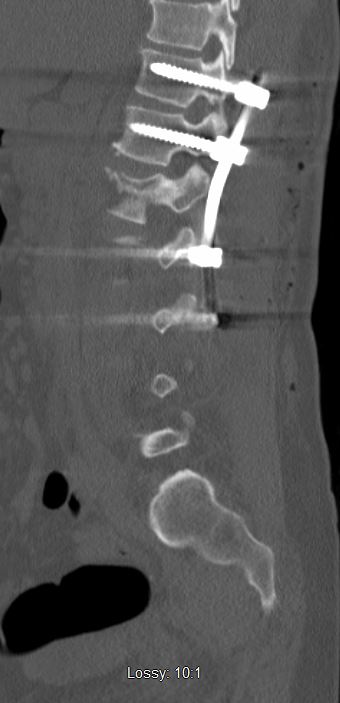
Not sure how others feel about this, but I’m ok with the inferior endplates no aligning all the time. If we look at the lateral image for this level the superior and inferior endplates are not parallel. So if you change the C arm to coincide with one endplate the other endplate will not be.
So, if given the choice, I’d prefer the superior endplate to be aligned because while obtaining intraoperative images while advancing the Jamshidi or screw I can see if my trajectory is headed for a superior endplate breech. You may also notice that some levels have pretty big meniscuses, menisci? A meniscus is another target for Parallax our villain friend from physics class. Anyway those concavities in the endplates throw me off and make the images look weird sometimes since it makes it harder to align the C arm to a surface that is not flat. It’s also sometimes hard to see pedicles due to fractures, positioning, body habitus, or osteoporosis. I don’t have great answers for you on how to improve visualization. I think those might be good cases for navigated screws with O arm? Then you can just get screws in on one try instead of the possible multiple attempts in osteoporotic or fractured bone. Navigated screws are fun too, they feel like a video game. Maybe more on navigated screws in another post.
